
Depressed Acne Scars ⋅ Acne Scars
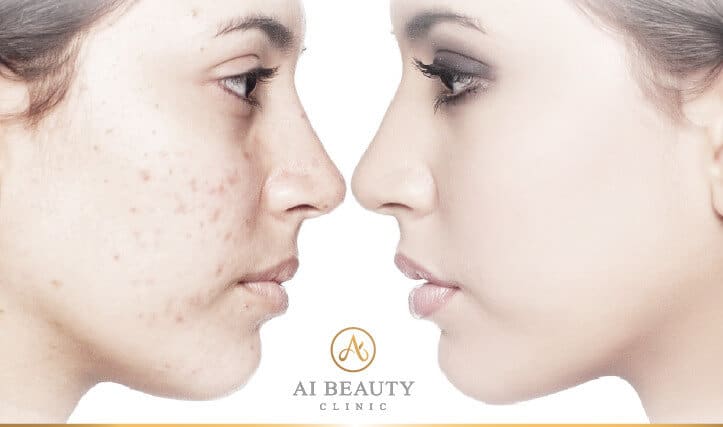
Compared to acne marks, it is more challenging to get rid of depressed acne scars because of its physical features. A face recovered from acne outbreak and left with depressed acne scars may look like the surface of the moon, causing distress and low esteem. However, aesthetic treatments could put an end to it!

What is acne scar
Acne scar is the scar left on the skin after the recovery of an acne. The scar can be developed as an atrophic (depressed) acne scar or a hypertrophic (raised) acne scar.

Depressed / atrophic acne scar shows depressions or indentations around the poles in the skin. The skin with depressed scars often has a rough texture and large pores and they are sometimes the results of popping the pimples.

Raised acne scar is ahypertrophic acne scar that leaves a red bumpy surface on the skin after recovery from acne. Sometimes, the scar may continue to grow when it is stimulated.
Causes
Inflamed acne or popping pimples inappropriately can lead to the formation of acne scars. Without a timely and appropriate acne treatment can result in inflammation of acne and damage and loss of skin tissue, creating uneven and depressed areas in the skin.

● Depressed acne scar is the result of the damage and loss of collagen due to the inflamed acne. The loss of collagen and the failure of collagen regeneration create depressed areas of the skin. Also, popping your pimples can cause the formation of depressed scars.
● Hypertrophic acne scar is also the result of inflammatory acne. It is formed when scar tissue forms on the skin in excess, as a result of excess collagen production, creating a bumpy scar.

◎Why popping pimples will lead to scarring?
When acne first occurs, the hair follicle is dealing with dirt, sebum, and bacteria, making it under a fragile condition. If you try to pop the acne, the pressure from popping may damage the skin underneath, leading to the infection at the dermis. Once the dermis is infected and damaged, the dermal tissue will start the self-healing process to replace the lost tissue. However, the process can be too slow or overly responsive, resulting in depressed acne scar and hypertrophic acne scars respectively.
On the other hand, leaving acne untreated or covering acne up with makeup can lead to acne scarring.
Symptoms
Generally speaking, acne scar can be divided into atrophic and hypertrophic:
- Depressed acne scar (Atrophic)

① Ice Pick Scar
Ice-pick acne scars are common scars that are deep, small, and narrow. They often show small, empty pores on the skin with obvious depressions.
② Boxcar Scar
Boxcar scars give the skin an uneven, pitted appearance. The pits are in various sizes with obvious depressions.
③ Rolling Scar
Rolling scars show broader and shallow depressions compared to other depressed scars.
- Raised Acne Scar

① Raised Acne Scar
When the dermis is damaged, the proliferation of fibroblasts in the dermis are stimulated to heal the wound. When the skin overreacts and forms excessive tissue on the wound, a raised scar will occur. A raised acne scar is difficult to get rid of through natural process, it appears as in red colour, hard texture, and a bumpy skin surface. Sometimes, the scar will be itchy and continue to grow and spread under external pressure or stimulation.
Affected people
People with oily acne-prone skin; People have long-term problem of acne; People who pop their pimples; People often have acne scar on their chin or chest; People who have depressed acne scars;
Treatment
Once depressed acne scars or raised acne scars are formed, it is difficult to remove them by simply applying cosmetic products. Alternatively, come to Ai Beauty Clinic, get to know about the medical beauty treatments such as laser, RF that are promising in treating these permanent scars.
A. Radiofrequency (RF) Microneedling
What is Radiofrequency (RF) Microneedling:
Radiofrequency (RF) Microneedling is an innovative technology integrating matrix application, microneedling, and radio frequency technology. During the treatment, a device with fine needles creates tiny punctures in the skin. The RF energy is then delivered via the small needles into the dermis to stimulate the production of new collagen and elastin. Results can include improved skin texture and firmness, as well as skin resurfacing.
How does it work:
A sterile treatment tip with a matrix of non-insulated, 24k gold-plated microneedles is used to mechanically and biologically stimulate the skin’s natural healing process. During the treatment, microneedles will be precisely inserted into the skin, and 1 million Hz frequency energy will be transmitted from the microneedles to the skin. The energy will penetrate the epidermis and reach the dermis layer, heating up the collagen fibres at the dermis to 55℃-65℃. The high temperature will damage the sebaceous glands and kill acne-causing bacteria, which can help reduce the pore size, inhibit the development of acne, control oil secretion and improve acne problem.
Procedure:
1. VISIA examination: Access skin condition or existing skin problems with assistance of data analysis and picture analysis.
2. Face-to-face consultation: Develop unique treatment plan based on client’s condition and desired results.
3. Apply anesthetic: Apply anesthetic externally. Clean and disinfect the treatment areas.
4. Pre-treatment preparation: Draw markings on the face to define treatment areas. Confirm the package of the new tip of the applicator has not been opened.
5. During the treatment: Perform the treatment as planned, precisely adjust the RF energy output and depth.
6. Post-treatment repair: Medical-grade facial repair mask + QDEL phototherapy mask to nourish and repair the skin.
7. Post-treatment care.
Duration: 1-1.5 hrs
Who is it for:
- People who have a severe problem of acne scars;
- People who have a serious condition of large pores;
- People with acne scars;
- People who have large pores problem that can not be improved by entrance level aesthetic treatments such as Mesotherapy or Photorejuvenation;

B. PicoSure Laser Pigmentation Treatment
What is PicoSure:
PicoSure is an aesthetic picosecond laser treatment that can safely and effectively remove tattoos and pigmentation. It has been certified by the US FDA and China CFDA and approved for the use in treatment of pigmented skin problems and pigmentation. A specific wavelength of light (755nm) is used to remove melanin safely, precisely and effectively.The PicoSure Laser device is equipped with a unique FOCUS lens. The FOCUS lens will redistribute 70% of the emitted laser energy and concentrate the energy into the skin, which will break down the melanin at the epidermis. The energy will also create a shock-wave hitting the deep dermis layer and damage the collagen, which will stimulate the repair and regrowth of collagen. Therefore, PicoSure treatment is not limited to improving pigmentation, but also smoothing lines, reducing pore size and restoring a youthful look.
How does it work:
During the rapid breakdown of melanin molecules, The equipped FOCUS lens will create a laser induced optical breakdown (LIOB) in the dermis to stimulate the repair and regrowth of collagen, which helps to brighten skin, reduce pore size, and remove wrinkles. The new collagen will fill up the depressed acne areas, restoring an even, smooth skin surface.
Procedure:
1. VISIA examination: Access skin condition or existing skin problems with assistance of data analysis and picture analysis.
2. Face-to-face consultation: Develop a unique treatment plan based on the client’s skin condition and desired results.
3. PATCH TEST: Perform a patch test 24 hrs prior the treatment. Proceed with the treatment when no allergy or abnormal sign is shown.
4. Pre-treatment preparation: Clean, disinfect and apply anaesthetics at the treatment areas. Put on safety goggles.
5. During the treatment: Deliver wavelength pulse at the pigmented areas, repeat steps at the severe pigmented areas. Cooling effect from cold air outlets.
6. Post-treatment: Apply aloe vera gel to soothe and calm down the treated areas.
7. Post-treatment caring.
Duration: 1-1.5 hrs
Who is it for:
- People with pigmentation and stubborn pigmentation;
- People with photo-ageing;
- People with lots of acne scars and pigmentation;
- People who want to improve acne scars, improve skin texture and reduce pores;

C. Mesotherapy
What is Mesotherapy:
Our skin is facing all kinds of damages everyday, like photodamage, pollution and the natural aging process. Mesotherapy can be a regular skin rejuvenation treatment that helps maintain our skin in a good condition in the long run. It is a non-surgical treatment that injects solution with various vital nutrients to our skin directly, which has a significantly higher absorption of nutrients than using skincare products. According to the skin condition, the injection content can also be tailored to meet one’s need for the maximum desired outcome.
How does it work:
Mesotherapy involves the injection of hyaluronic acid or/and multiple nutrients to the dermis. Dermis cells absorb the nutrients via osmotic absorption, which will activate cellular activity, promote the proliferation of collagen and elastic fibroblasts, resulting in smoothing depressed scars, improving pigmentation, deep hydrating and smoothing wrinkles. Leaving you a thoroughly improved skin texture, healthier skin condition and a perfect silky skin.
Procedure:
1. VISIA skin evaluation: Evaluate skin condition or existing skin problems with assistance of data analysis and picture analysis.
2. Face-to-face consultation: Tailored a suitable mesotherapy treatment plan based on client’s conditions and desired results.
3. Pre-treatment preparation: Apply anesthetics. Clean and disinfect the whole face.
4. Treatment: Administer injection solution by qualified practitioner. Repeat injection or scatter injection in severe areas.
5. Post-treatment care: Medical-grade facial repair mask and QDEL phototherapy mask to nourish and repair the skin.
5. Post-treatment precautions.
Duration: 60 mins
Who is it for:
- People who have dry skin;
- People with mild, shallow (depressed) acne scars;
- People who are looking for regular skin conditioning treatment to improve their irritated and rough skin;
- People who want to rejuvenate their skin;

D.Platelet-rich plasma (PRP) Treatment
What is Platelet-rich plasma (PRP) Treatment :
A Platelet Rich Plasma (PRP) treatment, also known as the “Vampire face-lift”, is an advanced treatment for skin rejuvenation purposes. The treatment involves the extraction of the platelets and white blood cells from the client’s blood via centrifugation. The resulting extract containing a high concentration of growth factors will be injected into the client’s skin. PRP treatment is a safe skin rejuvenation treatment that has obtained European CE, ISO and SQS certifications, and has been clinically proven by extensive research worldwide.
How does it work:
During the treatment, a small amount of blood is taken from your vein. The blood sample will be placed in a centrifuge that will concentrate the platelets and white blood cells in the blood. As a result, a PRP containing a high concentration of growth factors from your blood is obtained for your PRP treatment. The collected solution will then be injected into the client’s superficial dermis. The growth factors stimulate the regeneration and renewal of tissue, healing the damaged and aged cells, which will improve the skin texture, firm and lift the skin, reduce the appearance of wrinkles and depressed scars, restore a youthful skin condition and slow down the ageing process. Receiving regular PRP treatment can strengthen the skin defence system and heal the barrier ability in the dermis, restoring a healthier, youthful, and stronger skin.
Procedure:
1. VISIA skin evaluation: Evaluate skin condition or existing skin problems with assistance of data analysis and picture analysis.
2. Face-to-face consultation: Develop a unique PRP plan based on the client’s condition and desired results.
3. Pre-treatment preparation: Take blood from the client and obtain a concentrated platelet solution by centrifugation; apply anaesthetics, clean and disinfect the whole face.
4. PRP injection: Administer injection solution by qualified practitioner. Repeat injection or scatter injection in severe areas.
5. Post-treatment care: Medical-grade facial repair mask and QDEL phototherapy mask to nourish and repair the skin.
6. Post-treatment precautions.
Duration: 60 mins
Who is it for:
- People with mild, shallow (depressed) acne scars;
- People who are prone to facial redness and have pigmentation;
- People who have dull skin, textured skin and large pore;
- People who have damaged skin barrier;
- People who want to combine PRP with Mesotherapy as regular skin conditioning treatment;
E.M22 IPL treatment
What is M22:
M22 is an innovative photoelectric skin revitalisation instrument jointly developed by Lumenis, Stanford University, and Harvard University. It innovatively combines the world leading technologies (OPT technology and fractional non-ablative technology – RESURFX) to effectively treat pigmented lesions, acne scars, surgical scars, stretch marks, swelling lines, skin reconstruction (including reducing pores size, hair removal, skin rejuvenation, skin whitening, moisturising, etc.), facial lifting, and wrinkle removal. M22 has obtained the US FDA and the EU CE certification and is the cutting-edge technology that delivers top skin rejuvenation treatment.
How does it work:
M22 IPL treatment adopts the core OPT technology and the only true fractional non-ablative technology, RESURFX. The emitted intense pulsed light penetrates the deep layers of the skin and reaches the melanin pigment and capillary vessels selectively. By absorbing the light energy, the melanin pigment will be decomposed while the capillary vessels will be closed and destructed without damaging the skin surface. The capillary vessels will thereafter disintegrate, and the facial redness will be improved. On the other hand, M22 can stimulate the regrowth of collagen to restore skin’s elasticity, remove fine lines, reduce pores size and smoothen the skin texture.
Procedure:
1. VISIA examination: Access skin condition or existing skin problems with assistance of data analysis and picture analysis.
2. Face-to-face consultation: Customise unique treatment plan based on individual’s skin condition and desired results.
3. Pre-treatment preparation: Clean and disinfect the treatment areas. Put on safety goggles and apply treatment gel.
4. During treatment: Full face treatment, repeat steps at severe areas.
5. Post-treatment: Remove the gel, clean the face and apply a medical grade repair mask to calm the face.
6. Post-treatment caring.
Duration: 45-60 mins
Who is it for:
- People with red or black acne scars;
- People with mild (depressed) acne scars;
- People who have problems of pigmentation;
- People with photo-damaged skin;
- People who have chronic problems of facial redness and severe capillary vessels condition;
- People who want to brighten and juvenate their skin;

F. Acid Peel
What is acid peel:
Acid peel is a skin resurfacing procedure involving application of acidic solution on the skin. The acidic solution dissolves the oil particles among cells on the outermost layer of the epidermis and promotes the removal of the outermost layer. It stimulates the renewal of skin cells, promotes the replacement of elastic fibers in the dermis, and maintains the healthy state of the skin. It also helps with skin whitening, removing acne marks, reducing pores size and fine lines, removing blackheads, and curing acne and chloasma.
How does acid peel work:
Acid peel/AHA peel solution can loosen the physical attachment among stratum corneum cells by dissolving the oil particles between their cellular gaps, which will peel off the excessively accumulated keratin, unblock the clogged hair follicles and prevent the development of clogging opening at hair follicles. In addition, it stimulates the regeneration ability of epidermal cells and promotes dermal collagen fiber proliferation and its structural rearrangement, which will help to effectively improve skin texture (especially chicken skin), minimise large pores (by inhibiting oil secretion) and brighten skin tone.
Procedure:
1. VISIA examination: Access skin condition or existing skin problems with assistance of data analysis and picture analysis.
2. Face-to-face consultation: Provide suitable acid peel treatment plan based on client’s needs and goals.
3. Pre-treatment: Clean and disinfect the treatment areas.
4. Treatment: Apply an acidic solution on the face, waiting 1-5 mins.
5. End of treatment: Apply a neutraliser solution on face to terminate the acidic reaction and peeling reaction to avoid over peeling.
6. Cleaning. Post-treatment care.
Duration: 45-60 mins
Who is it for:
- People with acne-prone skin or oily acne-prone skin;
- People with mild, shallow (depressed) acne scars;
- People who want to brighten their skin tone;
- People who want to combine acid peel treatment with PicoSure or M22 Skin Photorejuvenation treatment to remove pigmentation and brighten skin tone;
- People who have acne scars alongside with closed comedone and large pores problems for long time;

E. Fotona 4D Pro
What is FOTONA 4D PRO:
FOTONA 4D PRO is the new-generation non-invasive anti-aging laser system for a comprehensive facial rejuvenation treatment. The system integrates the four patented modals: SMOOTHLIFTIN, FRAC3, PIANO and SUPERFICIAL to work on partial layers treatment and multi dimensional anti-aging solution, while simultaneously targeting different skin imperfections. It can treat four major ageing signs including contour, skin tone, skin texture and tissue volume in a safe and efficient way. FOTONA 4D PRO helps to restore a more youthful, more defined and rejuvenating appearance. In only 20 minutes, it resolves the imperfections around the eyes area including eye bags, wrinkles, puffiness, dark eye rings, etc.
How does it work:
Under the SUPERFICIAL micro skin resurfacing modal, the Variable Square Pulse (VSP) technology is used to emit a 2940nm cold ablation erbium laser beam to the upper epidermis to facilitate skin resurfacing by penetrating topmost to bottom layers. The SUPERFICIAL modal is highly effective in reducing wrinkles on the epidermis, correcting skin imperfections such as enlarged pores, blackheads and acne scars, as well as evening out skin tone and complexion. Also, the cold ablation procedure does not cause any damage to the epidermis.
Procedure:
1. VISIA examination: Access skin condition or existing skin problems with assistance of scientific tools.
2. Face-to-face consultation: Customise unique treatment plan based on client’s condition and desired results.
3. PATCH TEST: Perform a patch test 24 hrs prior to the treatment. Proceed with the treatment when no allergy or abnormal reaction is shown.
4. Apply anaesthetics: Apply anaesthetics externally. Clean and disinfect the treatment areas.
5. Pre-treatment preparation: Draw treatment areas to mark the treatment areas. Confirm the package of the new tip of the applicator has not been opened.
6. During treatment: Proceed with the scheduled treatment plan with flexibility to adjust the laser energy and depth.
7. Post-treatment repair: Medical-grade facial repair mask and QDEL phototherapy mask to nourish and repair the skin.
8. Post-treatment precautions.
Duration:30-45 mins
Who is it for:
- People with enlarged pores and acne scars;
- People with rough, unstable skin;
- People who want to heal and improve acne scars, improve signs of ageing, and rejuvenate their skin;
Improve acne scars, come to Ai Beauty Clinic,
for safe and professional medical treatment.

Ai Beauty Clinic is a CQC accredited clinic based in London, and also is strongly supported by Cynosure(the owner of Ulthreapy) and Cynosure (the owner of PicoSure).
With rich experience of treating clients of various conditions, led by a famous British medical chief trainer, practiced by doctors and nurses who are GMC/NMC-registered and worked in NHS national hospitals, Ai Beauty provides certified and safe medical beauty treatments.
Ai Beauty always puts safety first. Not only are all medical staff insured by independent medical policy, each client who comes to Ai Beauty Clinic is also insured by £5 millions medical insurance. This full insurance coverage allows clients to have a concern-free treatment experience.
Ai Beauty Clinic has served over 15,000 clients from all around the world, been covered by some famous media such as European Times and CW Television, and established trust and an excellent reputation among them.